Thursday, September 14, 2017 | Larry Sobal

For many health care organizations this is strategic planning and budgeting season. As I facilitate strategic planning retreats for hospitals, health systems, physician practices, and for their heart programs and cardiovascular service lines, I ask participants to write down what they think their number-one strategic priority is. As you can imagine, it’s not unusual to get multiple answers. So, I’ll usually follow that question with a request to write down how many number-one priorities people feel they currently have. Responses range from 3 to 100 (literally).
Just as heart disease can be a silent killer of people, lack of prioritization can become a silent killer of organizations. Health care leaders have many stakeholders inside and outside their organization, all approaching the leadership table with seemingly very important things to change or accomplish. Leadership often feels compelled to placate those stakeholders by proclaiming the need to act on all of those initiatives and assignments.
The result is overcommitment and overburden. Overburden is a phenomenon in which an organization asks its departments to pursue, often with equal amounts of urgency, a series of “critical activities” with more effort than is appropriate, available and warranted.
With the constant volley of new, competing, and sometimes conflicting initiatives swirling around, it is common that all initiatives are treated with equal importance. This reaction is fully owned by the leadership in each organization, as they are ultimately responsible for aligning initiatives to strategic goals and then finding the human resource capacity to execute and complete them.
It’s not hard to imagine health care administrative and physician leaders being as overwhelmed as the rest of the organization. The key difference is that they are the only ones who can lead the organization on a path that reduces the overburden.
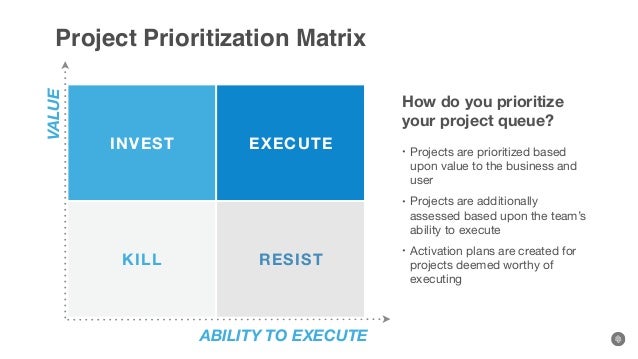
Harvard Business School professor Michael Porter has a famous quote: “The essence of strategy is choosing what not to do.” In other words, it’s about prioritization. Fortunately, there are a variety of tools to help you prioritize your priorities. Following are a few I often recommend to clients.
But prioritization is just one aspect of achieving a successful strategy. Some strategy gurus believe that an organization has a better chance of survival if it has a poor strategy implemented well, rather than an excellent strategy implemented poorly. In this day and age, hospitals and physicians likely don’t have the luxury of either. Building a sustainable health care system requires both a well-planned strategy and excellent implementation. Prioritization helps relieve resources from being overburdened, giving them a chance to be allocated to the most important strategies.
Just as heart disease can be a silent killer of people, lack of prioritization can become a silent killer of organizations.
Here are some other helpful tools and processes to use in your strategic planning process.
I have found almost all organizations are challenged with too many competing priorities. There will always be more good ideas than there is the capacity to execute them. In order to achieve something you have never achieved before, you must do things you have never done before. This requires a combination of disciplined focus, behavioral change and utilizing different leadership approaches. Once you adopt these change and execution principles, you will never lead in the same way again. And your strategy will stand a better chance of actually accomplishing measureable and meaningful change.
Illustration: Lee Sauer
 Larry Sobal is Executive Vice President and a Senior Consultant at MedAxiom. He has a 35-year background as a senior executive in medical group leadership, hospital leadership and health insurance. Larry consults, writes and presents on topics relevant to transforming physician practices and health systems. His weekly blog post comes out on Thursdays and can be accessed at www.medaxiom.com.
Larry Sobal is Executive Vice President and a Senior Consultant at MedAxiom. He has a 35-year background as a senior executive in medical group leadership, hospital leadership and health insurance. Larry consults, writes and presents on topics relevant to transforming physician practices and health systems. His weekly blog post comes out on Thursdays and can be accessed at www.medaxiom.com.
.


Larry Sobal, MBA, MHA, is CEO of a yet-to-be-named cardiology practice which is transitioning from employment to an independent physician group effective January 1, 2019. He has a 37-year background as a senior executive in physician practices, consulting, medical group leadership, hospital leadership and health insurance.
To contact, email: [email protected]
By continuing to use our site, you agree to our Cookie Policy, Privacy Policy and Terms of Use.
{kind=link}
Leave a Comment